

Commonly Treated Low Back Diagnoses
![]()
Strains & sprains, degenerative disc disease, leaky disc syndrome, disc bulges, disc herniations, spinal stenosis, facet joint pain, spondylosis, spondylolisthesis, spondylolysis, radiculopathy (pinched nerves), sacroiliac joint pain

The lumbar spine (low back) is the most common region of the spine to experience symptoms. The lumbar spine (shown in video) is vulnerable because it consists of a string of 5 vertebra that span between two large regions of the body, which generate significant forces on the lumbar spine – the torso above and the pelvis below. Low back muscles can become painful due to injury (strain) or due to the imbalance between muscles groups. Soft tissue symptoms related to muscle pain usually resolve rapidly with treatment or even resolve spontaneously without treatment. Chronic lumbar pain persists, however, and can be caused by any of the anatomical structures that constitute the low back.
Lumbar Disc Pain
![]()
Because the discs are located in the front of the spine, disc pain classically worsens while sitting and improves while standing. Disc pain can be felt in the low back or can refer pain into the buttock region and even into the back of the thighs. This referred disc pain can be felt on one side or both. The typical evolution of disc pain over time is that the flare-up episodes begin to occur more frequently, last longer and the associated pain becomes more intense. Eventually the situation can progress to constant daily lumbar disc pain with superimposed flare-ups. This process often interferes with activities, erodes quality of life, causes frustration and often leads to desperation.


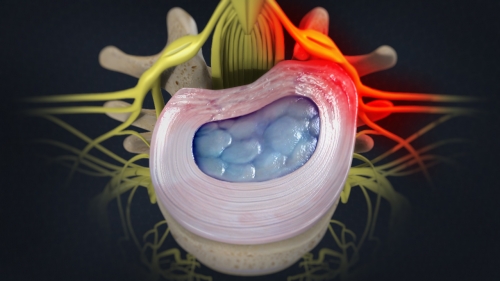
Lumbar Disc Annulus Tears (fissures)
![]()
The center of the disc is called the nucleus pulposus and has a gel-like consistency. The outer ring of the disc is called the annulus fibrosus and has a sturdier, but still flexible structure. Due to injury or degeneration, cracks (fissures) start to develop in our discs from the inside out. These cracks are called fissures and often correlate on an MRI with a high intensity zone (HIZ) visible in the disc annulus. Sometimes MRI reports call these disc abnormalities “annular fissures” or “annular rents”. Because the disc lacks an adequate blood supply, these disc annulus fissures cannot heal spontaneously. As a result, disc annulus fissures extend in length and become more numerous with additional branching complexity over time. The discs themselves can become painful because of this process.
Lumbar Disc Bulge & Protrusion
![]()
As more disc fissures form and progress, the disc annulus is weakened causing it to be displaced beyond its typical boundaries. If the disc annulus displacement involves less than 90 degrees of the disc circumference then it is called a disc protrusion, however, if the disc displacement involves greater than 90 degrees of the disc circumference then it is called a disc bulge. In order for a disc protrusion or a disc bulge to be present, there must be disc annulus fissures present to cause the disc wall weakening.

Lumbar Leaky Disc Syndrome
![]()
This term was coined by Kevin Pauza, MD and captures well the concept of what is occurring in the disc. When disc annulus fissures extend long enough to travel through the entire thickness of the disc annulus, then certain molecules can leak out of the center of the disc (nucleus pulposus), through the disc annulus fissures and into the epidural space, which is where spinal nerves are located. These leaking molecules trigger a series of chemical reactions that result in inflammation, which is irritating to nerve tissue. This inflammatory process can cause nerve pain symptoms in the corresponding leg even without any MRI evidence of a compressed “pinched” nerve.
Lumbar Disc Herniation & Extrusion
![]()
Disc fissures that have extended in length completely through the disc annulus can also widen, which allows material from the disc nucleus to escape outside the disc wall and result in a herniated nucleus pulposus (HNP). Depending on the shape and configuration of the escaped disc nucleus material, the abnormality on MRI is either called a herniation or an extrusion. This process causes not only inflammation around the spine nerves, but it can also cause compression upon them.


Lumbar Degenerative Disc Disease
![]()
Degenerative disc disease (DDD) can sound like an intimidating diagnosis, but in reality it is not a “disease”. Degenerative disc disease (shown in video) is actually a process that begins when tears (fissures) start to form in the outer wall (annulus fibrosus) of the disc, caused either by repetitive bending, twisting and lifting over time or the result of a specific injury. Because the disc lacks an adequate blood supply, the tears in the disc annulus cannot heal on their own. As a result they extend in length and become more numerous with additional branching complexity over time. Eventually these tears reach the outermost portion of the disc annulus, causing them to leak over time. The center of the disc (nucleus pulposus) eventually loses enough of its fluid content causing the disc to decrease in height and eventually collapse. On MRI these discs appear dark and flat compared to discs that are not degenerating.
Spinal Stenosis
![]()
As the discs get progressively flatter the vertebral bones surrounding the disc move closer together, which causes slack (laxity) in the supporting ligaments that connect one vertebral bone to the other. The body responds to this ligament laxity by reinforcing the area with calcium deposits called osteophytes (bone spurs). As these osteophytes grow they eventually cause other spine problems by progressively narrowing the channels through which nerves of the spine travel. This narrowing process is called lumbar spinal stenosis (shown in video) and can involve narrowing of the vertebral canal, the intervertebral foramen or both regions. It is important to recognize that this entire degenerative disc disease process begins with disc annulus fissures.

![]()
Lumbar Disc Treatment

All of the traditional nonsurgical treatment options are first considered and discussed: activity modification, independent exercises, formal physical therapy programs, braces, medications or other treatment interventions. Inflammatory irritation can result from all of the disc abnormalities: disc annulus fissures, leaky disc syndrome, disc protrusion/bulge, disc herniation/extrusion or degenerative disc disease. When inflammatory nerve symptoms (“pinched nerve”, sciatica) are associated with an underlying disc condition then a lumbar epidural steroid injection (shown in video) using fluoroscopic guidance is a consideration. The use of steroids in the epidural space is a common off label use for this class of medication, however doing so still remains an alternative for patients to consider, especially if their goal is to avoid spine surgery. Even though steroids can intervene with the inflammatory process in the epidural space, they are not capable of resolving the underlying disc problem, which involves the presence of fissures in the disc annulus. The Discseel® Procedure can be used the seal the tears in the discs.
Lumbar Facet Joint Pain
![]()
Facet joints are also called zygapophysial joints (z-joints). Because they are located in the back of the spine, facet joint pain classically worsens while standing and walking then improves while sitting. Facet joint pain (shown in video) can be felt in the low back or can refer pain into the buttock region and even into the back of the thighs. This referred facet joint pain can be felt on one side or both. Just like any joint in the body, each facet joint surface is covered with cartilage called articular cartilage, which allows the facet joint surfaces to glide smoothly over one another with minimal friction. Due to injury or degenerative wear and tear, this articular cartilage can deteriorate and cause arthritis pain symptoms. Pain messages from the painful joints are transmitted via small nerves called medial branches.


Lumbar Facet Joint Treatment
![]()
All of the traditional nonsurgical treatment options are first considered and discussed: activity modification, independent exercises, formal physical therapy programs, braces, medications or other treatment interventions. When facet joint symptoms persist despite appropriate conservative care then using fluoroscopic guidance to perform injections becomes an option to consider. A facet joint steroid injection can interrupt facet joint inflammatory pain symptoms associated with joint degeneration. A Lumbar Medial Branch Block (MBB) (shown in video) is a diagnostic injection that can verify to what degree spine symptoms can be attributed to the facet joints.
For facet joint pain symptoms that return despite these two injection approaches, then Lumbar Radiofrequency Ablation (RFA) Neurotomy (shown in video) of the corresponding medial branches can be a nonsurgical option to discuss. For individuals who prefer an alternative treatment approach to facet joint pain symptoms, then Regenerative Medicine options can be discussed like Bone Marrow Cell Theraphy or Platelet Rich Plasma (PRP) Theraphy.


Lumbar Spondylolisthesis
![]()
Arthritic degenerative changes in facet joints can alter their function. Ordinarily, facet joints permit one vertebra to “anchor” to its neighboring vertebra. As facet joint function becomes compromised, one vertebra can slide forward or backward relative to the neighboring vertebra – a process called spondylolisthesis. A stress fracture (spondylolysis) close to the facet joint can also result in spondylolisthesis. The treatment of spondylolisthesis depends on which symptoms are manifesting. The facet joints or the intervertebral disc can be painful due to the process of one vertebra sliding over the next. The process of spondylolisthesis can also place tension or compression on the nerve roots at that level the spine.
Sacroiliac Joint (SIJ) Pain
![]()
The sacroiliac joints are located in the back of the pelvis where the sacrum forms joints with the iliac bones of the pelvis. There is one SIJ on each side of the sacrum and these joints are a common cause of buttock pain, especially noticeable when transitioning from sitting to standing or the reverse. In the treatment of sacroiliac joint pain, all of the traditional nonsurgical treatment options are first considered and discussed: activity modification, independent exercises, formal physical therapy programs, medications, braces or other treatment interventions. When SIJ symptoms persist despite appropriate conservative care then a sacroiliac joint steroid injection (shown in video) using fluoroscopic guidance becomes an option to consider. If a sacroiliac joints symptoms persist or return then Regenerative Medicine options like Bone Marrow Cell Therapy or Platelet Rich Plasma (PRP) Therapy can be discussed.
